Genetic Disease Investigators LLC, Diana Driscoll, OD, President, is a global leader in autonomic research. The first to identify abnormalities of parasympathetic nerves (such as the vagus nerve), vascular problems, and intracranial pressure abnormalities, Genetic Disease Investigators LLC continues to release answers — years in advance of others.
Help us get answers! Sign up for a study today!
If you are a chronic dry eye patient interested in new treatments, we invite you to participate in these studies:
Dry Eye Survey:
Complete this 3-minute survey to see if your dry eyes could be more than just an “eye problem”.
This exciting new study will be treating dry eyes using NeuroTears./span> This ground-breaking research uses a patented over-the-counter supplement to stimulate both inflammation control and tear production simultaneously. Please let us know if you are interested and we will reach out to you to see if you qualify.
Let us know if you’re interested!
Latest Research The Future of Medicine Today
COVID and the Vagus Nerve – An amazing discovery
COVID and the Vagus Nerve – An amazing discovery By Dr. Diana Driscoll, Optometrist, FAAO The vagus nerve is affected in post-COVID Longhaulers! This…
Do You Need to Stimulate Your Vagus Nerve? What You May Be Missing! By Dr. Diana Driscoll, Optometrist The vagus nerve is the major nerve controlling the…
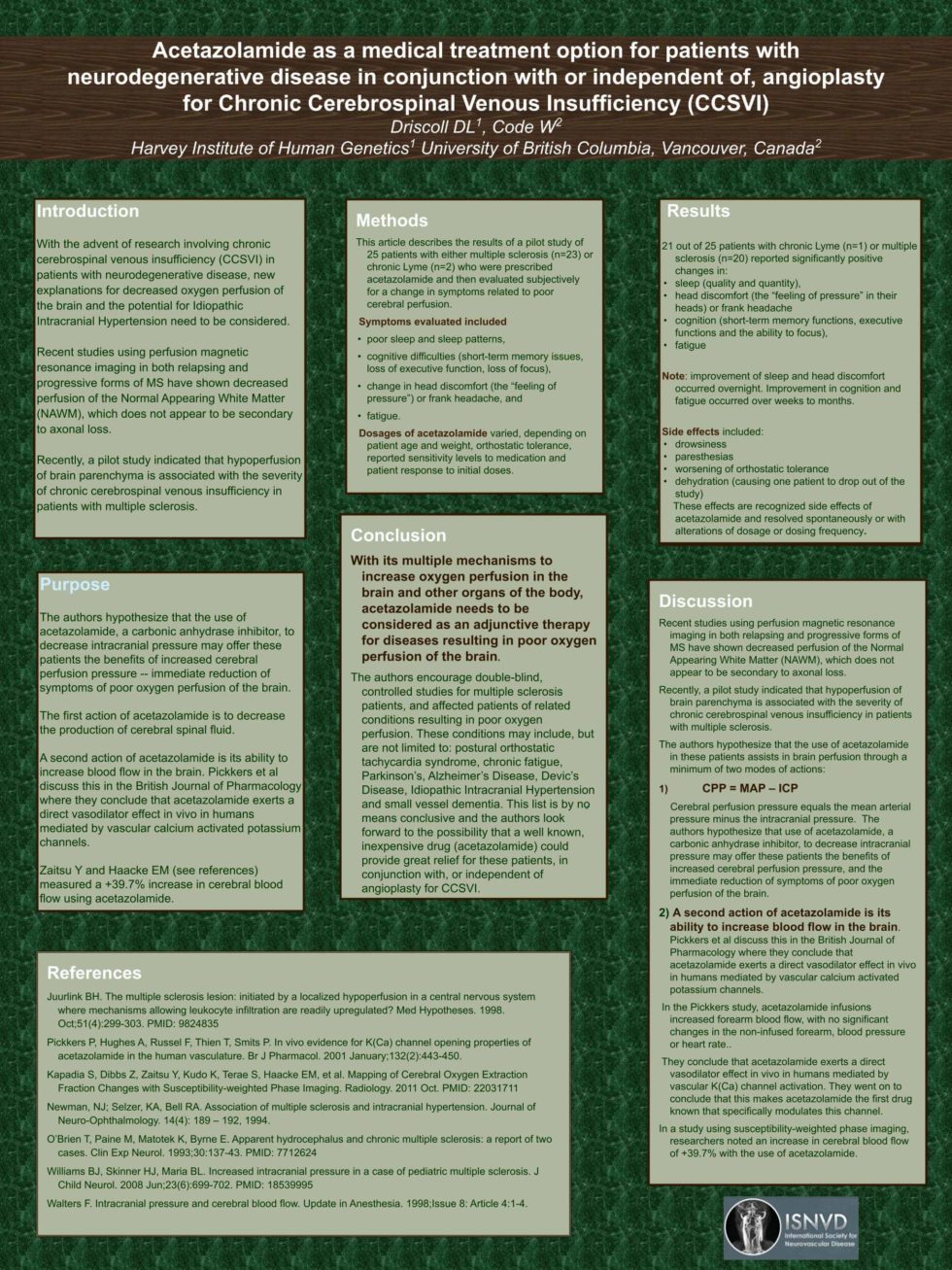
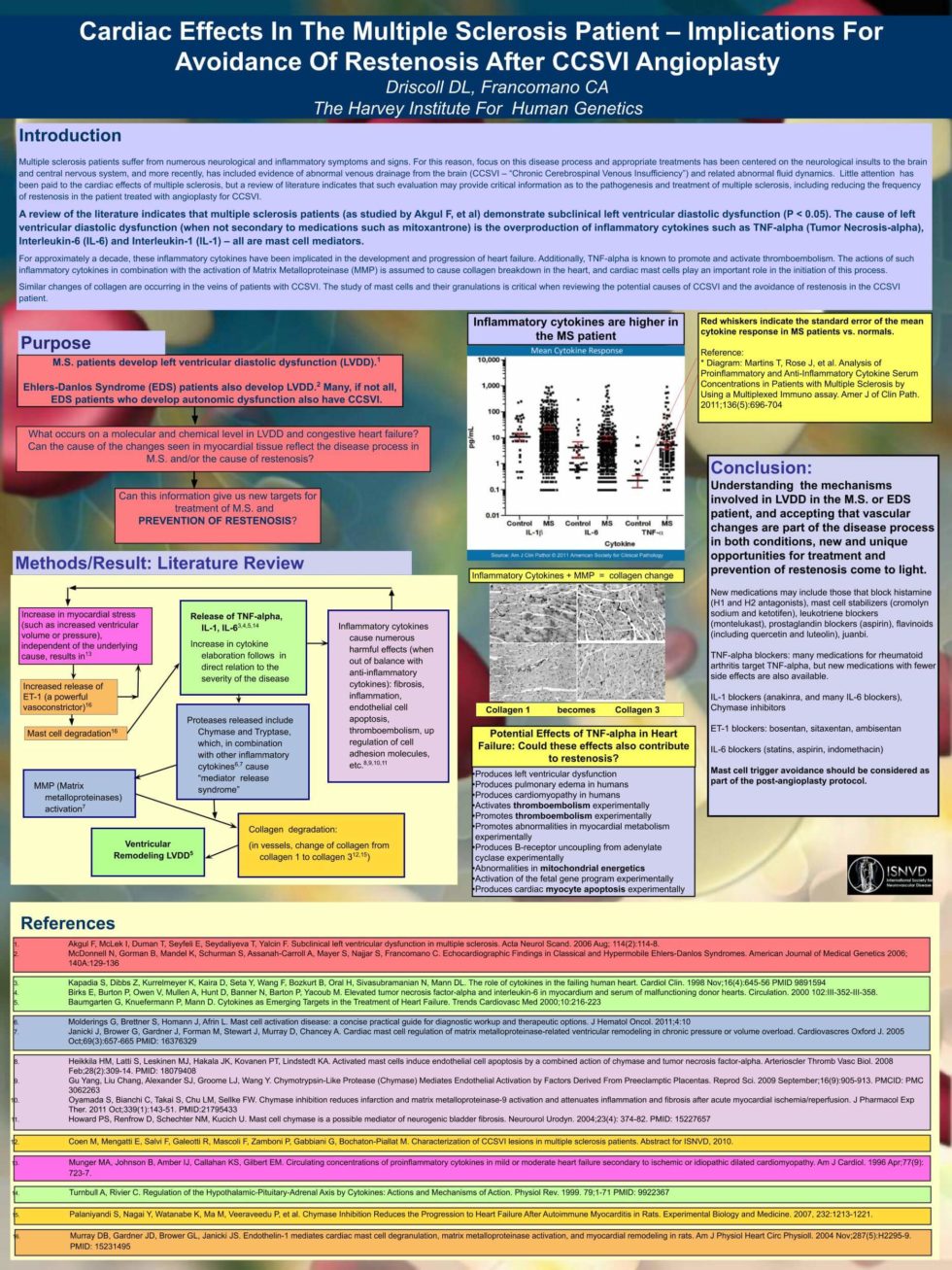
Acetazolomide as a medical treatment option for patients with neurodegenerative disease
Presented February 2012 — International Society of Neurovascular Disease This study, co-authored by Dr. William Code and Diana Driscoll, OD revealed the…
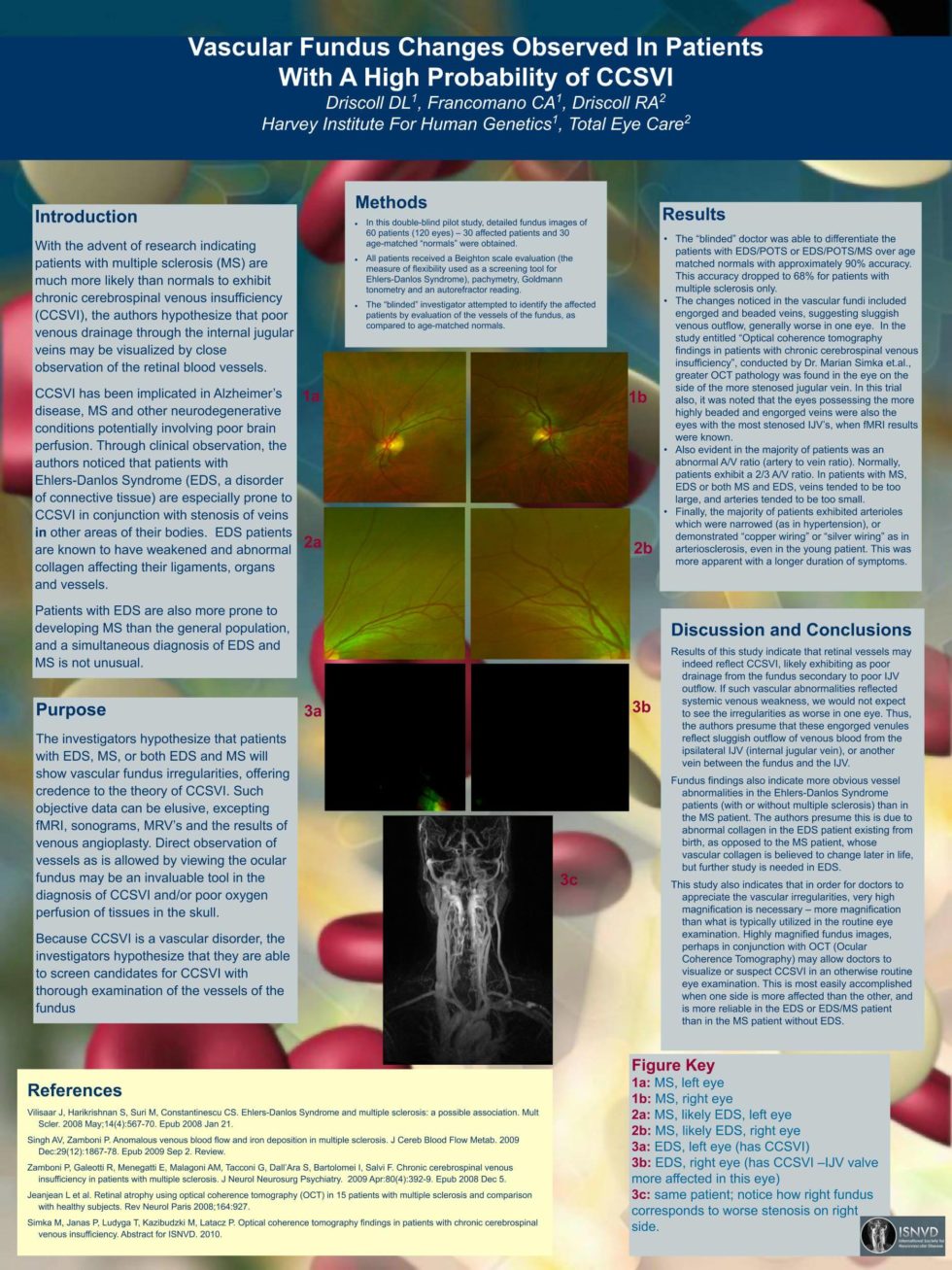
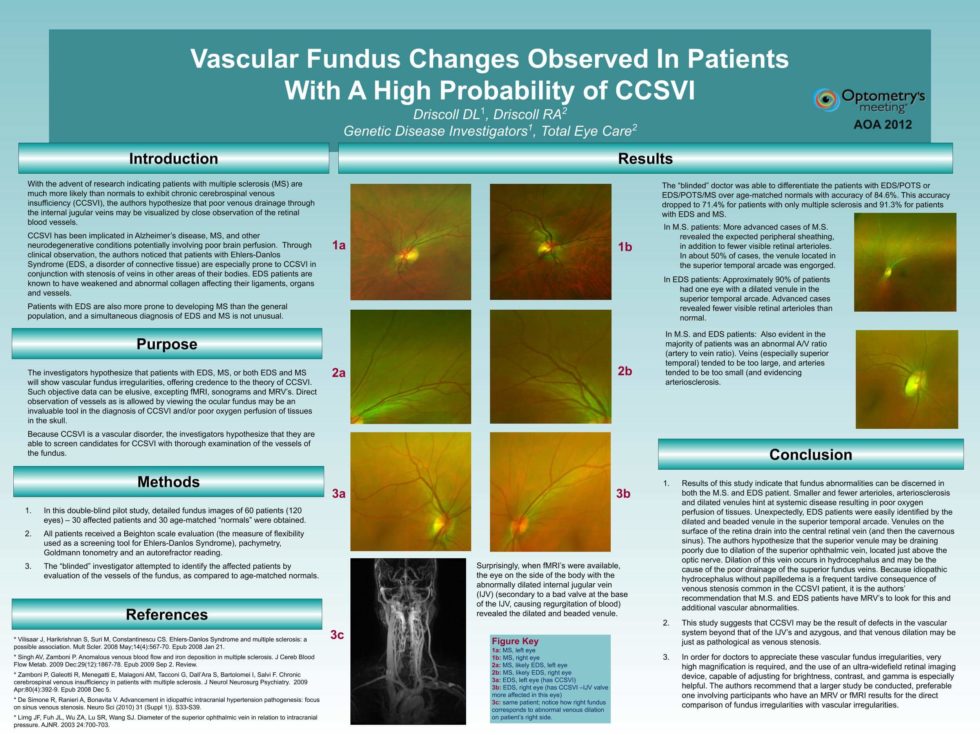
Vascular fundus changes in patients with high probability of chronic cerebrospinal venous insufficiency
June 2012- Optometry’s Meeting Clinicaltrials.org NCT#01356134 This study included co-authors Dr. Clair Francomano and Diana Driscoll, OD and involved the…
Head circumference growth in children with Ehlers-Danlos syndrome who developed dysautonomia later in life
Clinicaltrials.org NCT#01367977 Preliminary results of this study revealed abnormally fast growth of head circumferences (as opposed to the lengths and…
Evaluation of lipo(a) in patients with vascular fibrosis and EDS/POTS/Dysautonomia
An in-house study of six patients with EDS / POTS / Dysautonomia and vascular fibrosis run to find out if abnormal lipo(a) was the cause of their vascular…